In exams, ankle spotters are about quick identification. In radiology, they’re about recognizing instability, joint involvement, and what changes management.
The ankle is compact, but the logic is simple:
Is the joint stable? Is the articular surface involved? Is this something that needs surgery?
This guide focuses on high-yield patterns you should recognize instantly on X-ray and CT, and more importantly, how to think and report them.
1. Trimalleolar Fracture: Think Instability First
A trimalleolar fracture involves:
-
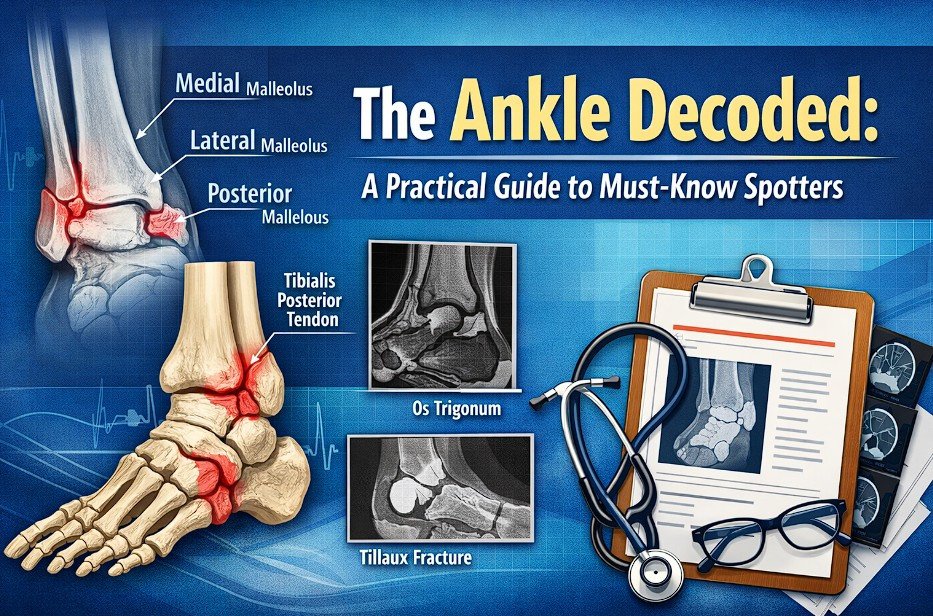
Medial malleolus
-
Lateral malleolus
-
Posterior malleolus
From a radiology standpoint, the key question is not “how many fragments,” but what does this do to the ankle mortise?
What to Look For on Imaging
-
Disruption of ankle mortise alignment
-
Posterior malleolar fragment size and displacement
-
Associated talar subluxation
Why the Posterior Malleolus Matters
This fragment contributes to the articular surface and syndesmotic stability.
If involved:
-
Instability is likely
-
Syndesmotic injury may coexist
-
Surgical fixation is often required
Reporting Line
“Trimalleolar fracture with involvement of posterior malleolus, associated with ankle mortise disruption and features of instability.”
2. Tibial Plafond (Pilon) Fractures: The Articular Injury
The tibial plafond forms the weight-bearing surface of the ankle joint.
Imaging Hallmarks
-
Comminution of distal tibia
-
Intra-articular extension
-
Impaction of articular surface
-
Associated fibular fracture (common)
Mechanism Insight
Axial loading drives the talus into the tibial plafond, crushing it.
Why It Matters
These are not just fractures. They are joint destruction injuries.
Expect:
-
Irregular articular surface
-
High risk of post-traumatic arthritis
Reporting Focus
-
Degree of comminution
-
Articular step-off
-
Alignment
-
Soft tissue status (on CT if available)
Reporting Line
“Comminuted intra-articular fracture of distal tibia involving the tibial plafond (pilon fracture) with articular surface disruption.”
3. Tillaux Fracture: Transitional Injury Pattern
Seen in adolescents with partially fused growth plates.
Imaging Features
-
Fracture through distal tibial epiphysis
-
Involvement of anterolateral aspect
-
Extension into the physis
-
No metaphyseal involvement (Type III)
Mechanism
External rotation force avulses the anterior inferior tibiofibular ligament insertion.
Why You Should Care
Even small displacement matters because:
-
It involves the joint surface
-
Malreduction leads to early arthritis
CT is often used to assess displacement.
Reporting Line
“Salter-Harris Type III fracture of distal tibia (Tillaux fracture) involving the anterolateral epiphysis with intra-articular extension.”
4. Os Trigonum: Don’t Overcall It
A common reporting pitfall.
Imaging Features
-
Small ossicle posterior to talus
-
Smooth, corticated margins
-
No adjacent fracture line
Key Differentiation
Fractures look irregular and lack cortication. The os trigonum looks like a finished structure, not a broken one.
When It Becomes Relevant
May be associated with posterior ankle impingement, especially in athletes.
Reporting Line
“Incidental os trigonum noted posterior to talus. No imaging features to suggest acute fracture.”
5. Peroneal Tubercle: Subtle but Useful
Located on the lateral calcaneus.
What to Assess
-
Prominence or hypertrophy
-
Relationship to peroneal tendons
Clinical Correlation
An enlarged tubercle can:
-
Cause tendon impingement
-
Lead to chronic lateral ankle pain
MRI is useful if tendon pathology is suspected.
Reporting Line
“Prominent peroneal tubercle with potential for peroneal tendon impingement. Clinical correlation advised.”
6. Tibialis Posterior Tendon: The Arch Indicator
This tendon is critical for medial arch support.
Imaging (MRI/US)
-
Tendon thickening or degeneration
-
Partial or complete tear
-
Associated medial arch collapse
Radiographic Clues (Indirect)
-
Flattening of medial arch
-
Hindfoot valgus
Why It Matters
Dysfunction leads to adult-acquired flatfoot, which progresses if untreated.
Reporting Line
“Features suggest tibialis posterior tendon dysfunction with associated medial arch collapse.”
How to Approach Any Ankle Spotter
Instead of memorizing labels, run a quick mental checklist:
-
Alignment – Is the mortise intact?
-
Articular surface – Is the joint involved?
-
Fragment significance – Does this affect stability?
-
Mechanism – Does the pattern make sense biomechanically?
-
Management implication – Does this likely need surgery?
If you answer these, you are no longer guessing. You are interpreting.
Takeaway
Ankle imaging becomes straightforward once you shift from naming structures to understanding stability and joint integrity.
-
Posterior malleolus → think instability
-
Plafond involvement → think joint damage
-
Growth plate injury → think long-term consequences
-
Accessory bones → avoid overcalling
Spotters test recognition. Radiology demands interpretation. Train for the second, and the first takes care of itself.